If all goes well my life as an ostomate comes to an end on Tuesday, April 9th when my ileostomy is reversed and my colon starts to be used again as God intended.
I would be lying if I said that life as an ostomate was easy. There were many challenges, the most difficult and dangerous one being dehydration. In fact, I ended up in the emergency room and a several day stay in the hospital about two weeks ago because of the norovirus and the fact that I didn’t realize I was having diarrhea until it was almost too late.
I had noticed during the day that my output was hiring than usual and that I was thirstier than normal. Because I happened to be at a church conference I more or less ignored this and kept attending to the business at hand. I was drinking, but I didn’t take any additional loperamide HCI (aka Imodium) or other medications that might have slowed down the fluid loss. By the early evening I was starting to feel a little unwell. So, I had some applesauce and rice krispies. I ate a banana, I took the loperamide and drank more water. But it was too late. Chills set in and then came the cramps.
It started with a leg cramp and I thought I had been sitting in the chair funny. So I tried to walk it off. Then the other leg cramped up, then my abdomen – I realized something was horribly wrong and thought I might actually be having another heart attack. So I went to the nearest phone by my bedside and reached for it as I collapsed into my bed thinking “Oh God, this is it.”
I woke up next to my bed, phone in my hand and buzzing at me, items from my nightstand scattered on the floor around me. I was so out of it I didn’t realize that I had actually passed out. I managed to call my sister, who was just getting home from helping my mother – who had also fallen ill (we surmised later that we both caught the norovirus from the same source).
We got to the emergency department of the University of Michigan Medical Center quickly. In hindsight we probably should have called an ambulance as the cramps hit again and I passed out not twenty feet from the entrance.
Pro-tip: want to pass by the waiting room at the Emergency Department? Pass out in their parking lot. I was whisked in pretty quickly. After receiving the excellent care that I am used to from Michigan Medicine I was re-hydrated and my cramps stopped. No cardiac event, but my kidneys had shut down from the stress – that’s how badly I was dehydrated.
Moral of the story?
Ostomates – always pay attention to your fluid intake and output. This can literally be a matter of life and death.
Everyone else – for pity’s sake wash you hands after using the restroom. Norovirus is easily spread in the most minute traces of fecal material. This spread is easily preventable by properly wetting your hands, sudsing with soap for an appropriate amount of time (try singing “Happy Birthday” to yourself a couple times) and drying. When you skip this step you may think you are somehow avoiding germs by not touching things in the bathroom, but you are making the rest of us sick when we shake your hand or come in contact with you later. Especially those of us with lowered resistance due to a compromised immune system. Like all of us with Crohn’s, Ulcerative Colitis, and who knows how many other invisible diseases and the medications we are on.
Please, please, wash your hands. The life you save might be mine!
I’ve learned a lot during my time as an ostomate and I have a greater appreciation and respect for those who cannot have theirs reversed. I hope in some small way I’ve helped you to better understand this experience as well.
Last year on Thanksgiving I hit my head while playing kick ball with my cousins (yeah, we’re not exactly the Kennedys). This led to me having an EKG and the discovery that sometime in the past that I had a heart attack, which led to changing my Crohn’s medication for fear it was effecting my heart function, which led to a bowel perforation and my current ostomy.
So what am I thankful this year? Just being alive and able to celebrate another Thanksgiving with loved ones!
Which may be as much as any of us should be thankful for.
So, in my constant quest for greater fitness I thought it might be fun to engage a couple friends in a challenge to see who could lose the most body fat in the next few months (by the start of spring). I decided that I should switch out my trusty Tanita scale that I’ve been using for some years with a Taylor scale that I’ve also been using on and off (to paraphrase that old saying: a man with one scale knows how much he weighs, a man with two is never sure). The reason being because though both scales measure body fat percentage – and are pretty close in their measurement – the Taylor scale has a few more
The Tanita and Taylor scales – both good
features including a calculation of hydration and muscle mass, all of which are uploadable into an app for easy tracking. For the challenge we have decided to use waist/hip ratio as our measurement tool, but I thought I’d follow my progress on the scales, too. Since I do weigh myself everyday anyway.
The “new” scale works nicely and as I said the body fat percentage corroborates with the other scale. But, today I took note of the other measurements. Fat mass was where I expected at about 25% (needs to be under 20), body water at 59% – a little dehydrated which isn’t surprising since my colon isn’t there absorbing water anymore since my ileostomy – and my muscle mass was at just over 30%. Now, you’ll notice that these percentages added together total more than 100%. I haven’t found it in the documentation yet, but I suspect that the body water figure is independent of the other two and is calculated off the remaining body mass (organs and skeleton). So, based on these readings my body is a little over half fat and muscle. So far so good right?
Well, I then wondered how my muscle mass compared with the average guy – you know, because we guys are all about measurements and comparisons with other men (to prove we’re better). Since I’ve been working out I’ve always assumed that I had more muscle
Me during my “glory” days
mass than most men. I know that my arms are larger, even now in their “depleted” state (a little over 15″ in circumference compared to the average untrained American male who is around 11″) they do flex and do not jiggle when I move them. I once benched 350 pounds and still am capable (I think) of a one time max of more than my bodyweight. Good for anyone, great for a man of my “advanced” years. Plus, you know, I have done squats in the past, too keeping my lower body pretty fit – even with too much fat around the hips (you should see the definition in my “marching band” calves).
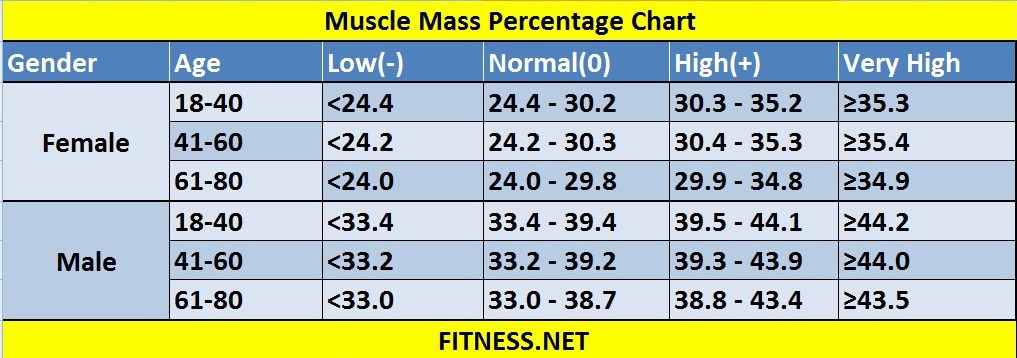
So off to Google I go and search for “how much muscle does the average man have” and imagine my surprise to find out that according to my scale I not only have less muscle than the average man (about 60 pounds compared to livestrong.com’s average of 72 pounds). I thought, “okay, but surely my percentage is higher.” Nope…
Not only am I low for the average man, I’m low for a man my age and older! How is this possible? I was only in the hospital for a week and recovery for six weeks. Can muscle mass be lost that quickly?
Now, I did come out of the hospital 20 pounds lighter than I went in. This would equate to a loss of about 2 pounds a day for my 10 day stay, but most of the weight loss was early. I never figured out why it was so much, as I doubt that a meter of intestine (the full length of my ileum) weighs that much since it’s essentially a hollow tube of muscle and skin. Maybe it was because of all the stuff that was leaking into my abdomen was no longer there, a lot probably water weight, and maybe an incidental “liposuction” when they cut through the fat and muscle to get to my innards. I just didn’t know. However, I felt that when I cam out that my chest and shoulders had disappeared on me. Could I
Me shortly after surgery in August 2018
really have lost that much muscle that quickly? Or is my scale wrong. Did one operation undo 30 years of weightlifting and bodybuilding?
I think it will be interesting to see what happens over the course of the next few weeks and months as I continue into my workout routine. I will admit that I wasn’t doing a lot prior to the operation but I was lifting twice a week and getting in some cardio. Plus, there was the cardio rehab I had just finished earlier in the late spring. Muscle memory is a wonderful thing, but we all know that as we get older we don’t bounce back as quickly as we did before.
In fact, most studies indicate that as we age we lose a significant amount of muscle with some, if I recall correctly, suggesting men lose as much as 10% of their muscle mass for each decade after 40 (or earlier). Most studies also suggest that this loss is as much due to inactivity as anything as we tend to move less as we get older and that working out becomes less of a priority when family and career get involved (thus the rise of the so-called “Dad Bod” someone with some muscle on them but it’s covered in a layer of fat).
However, there are also studies that suggest that this muscle loss can be slowed if not completely reversed. That, contrary to popular belief, even people in their eighties and nineties can gain muscle. Maybe not as fast as in our youth, but gains can be made. In fact, I feel that I was at my strongest in my mid to late forties. Not necessarily my fittest, just my strongest.
Which bring ups an interesting tangent. I had a conversation recently with a young man who I’ve befriended at work. He’s a bodybuilder (though I don’t think he would consider himself one since he lifts primarily for “fun,” but I’ve seen his before pictures and he’s clearly a bodybuilder) and he asked me an interesting question: “do you know how men keep getting stronger as they get older?” I replied that I had noticed the same thing myself, stating that many bodybuilders seem to hit their prime in their thirties and how I felt I gained strength well into my forties. But he then said, “no, do you know HOW men keep getting stronger?” and I indicated that I wasn’t sure, perhaps the body doesn’t actually fully mature until a man is in his twenties or later.
Now, I think I can answer that question a little better. Men who keep getting stronger as they age also don’t give up. They stay focused on being a little better each day, at lifting a little more, running a litter farther.
Basically, men get stronger as they age because they think they can.
As I sit here eating my lunch – because my appetite is still quite strong – I was thinking about a few things regarding my surgery and recovery. Thought I’d take a few minutes to share them because, why not?
Healing: the healing process is frustrating slow. Not regarding the stoma, that seems fine, but the darn incision. Most of the incision is healed and scarred (lovely) but a couple spots just don’t seem to want to close and keep oozing. Not blood, but exactly what you think of when you hear or read the word “ooze.” So, I’m changing dressing twice a day to keep up with the flow and trying not to get too grossed out when I do. Yesterday at the doctor’s office he essentially cauterized a couple areas of what he called “granulation.” When talking about skin healing, granulation is the process where new tissue is created to fill in the gaps of the wound. It starts from the base up, so for a deep wound it takes some time. However, in my case, I had a couple areas that overgrew and formed small lumps on the scar. These may have been infected so the cure was to remove them chemically and one by “snipping” it off. The Good News: If all goes well, my oozing should stop in about a week or at least dramatically slow. I’m looking forward to not changing dressing.
Output: I can’t seem to get the hang of regulating the output of my stoma. Everytime I think things are settling down – so I don’t have to empty out every hour – I backslide. I’ve discovered that lemonade is a problem so I have to avoid that. I’m taking imodium like it’s candy (up to four pills, four times a day), and have eaten enough toast, applesauce, bananas, and rice krispies to bind up an elephant! But, I’m spending more time in the bathroom now than before the surgery. The Good News: The doctor thinks I’m making progress and have the tools I need to get there. I’m not de-hydrated and my weight is stable. He thinks I look “great” so there’s that. Of course, he’s only seen me two times now (part of the post-surgery clinic).
Breakage and Leakage: not fun anytime, especially in the middle of the night or when out and about trying to do normal activities. The Good News: I seem to have re-gained the hang of when to change my appliance. No accidents for more than a week now (knock wood).
Enough venting. According to the doctor I’m free of all lifting and exercise restrictions. I plan to start working out – slowly – this week and get back to tap dancing again next week.
And, then there’s my trip to Florida in about two weeks…
Well, it’s been a little over a month since I became what is known as an “Ostomate.” This is a person who’s insides have been altered to create a new opening for his or her intestine to empty through (aka a stoma).
Hopefully, to assist the few other new ostomates who may stumble across this blog here are a few things I’ve learned so far. Some the doctors, nurses and dietitians warned me about. Most, they did not:
No matter how careful you are, no matter how often you empty your appliance, you will have accidents. It might be a leak or a blowout – but it will happen.
Some of these will occur at an inopportune time like work (once), before a social function (once), or in bed (three times so far).
Invest in a mattress cover. Don’t skimp on this. I got one that’s breathable and noiseless. Sheets can be cleaned. Mattresses, not so much.
Have emergency kits on hand in your car and at work (a pre-cut appliance, powder, solvent, whatever you need to make a change). I also have spare underwear hidden in my office.
Follow the doctors’ and nurses’ orders. I know, this should be a no-brainer, but it’s worth repeating.
Be patient. It takes a while to adjust to life with your new friend.
Try a pouch support of some kind. I have a band that I slip into with a built in pouch. Check on line there are several styles out there.
Guys, suspenders are better than belts.
Chew, chew, chew. The stomach is an amazing organ and very efficient at breaking down what you eat. But it can’t do it alone. Avoid “chunks” and chew carefully. Trust me on this.
Share your story with friends and family. My first instinct was to not let people know what I was going through. But, there are more of us than anyone realizes. It doesn’t help to keep it a secret.
Red dye is forever. Before you panic because you think your bag is filling with blood, take a deep breath and think, “what did I eat?” One popsicle or glass of Hawaiian Punch can put a very quick scare into you.
Having stated the above (#9), remember it’s okay to be discreet. I don’t tell everyone I meet that there something different about me.
You are going to learn a lot about how your food is digested. This can be interesting and disturbing at the same time. For example: fish smells like fish going in and coming out.
Try to focus on the positive of your situation. Is your pain from Crohn’s, Ulcerative Colitis, or whatever issue gone? Hemorrhoids cleared up? And I bet you don’t miss having to strain to relieve yourself anymore.
Don’t focus on what’s changed in your life, focus on what’s the same. Get back to your normal routine as quickly as you can and your energy allows. Remember, your life didn’t change – only your plumbing did!
Don’t get me wrong, I have my moments of despair and depression, too. I have times when I hate that this thing was done to me and that now I’m not “normal.” But, I then focus on why it was done – literally to save my life – and that perhaps I was spared by God for a greater purpose. I just need to figure out what that is.
You know, like everyone should.
Onward!
P.S. – you’ll also get really good at estimating how many milliliters of liquid there are in any container. You know why…
“Mr. Wahr, Mr. Wahr? Do you know what’s happening?” the young med student who just woke me at 4:00 A.M. asked me.
“I think so,” I replied. I had come in to the University of Michigan Hospital less than 24 hours earlier with abdominal pains that didn’t feel like a normal Crohn’s attack. Something was off so after much hemming and hawing I finally decided that given my heart history I really couldn’t take the chance that something was really wrong. Especially since the pains had started the day before and weren’t lessening as was the usual pattern with my Crohn’s, “but why don’t you tell me.”
She looked at me with sympathetic eyes and said, “you’re going in for emergency surgery. A surgeon will be in shortly to explain.” Surgery? I had certainly anticipated this. In the Emergency Department they had determined that I had what they called a “micro fissure” of the fistula in my ileum. But, at least at that time, they didn’t think I needed surgery within 12 hours. So I had been moved to a room for observation.
Almost as soon as she finished her sentence a young man appeared at my bedside – why are all doctors so young now? – in a polite, but firm tone he said, “Mr. Wahr, I’m sorry but you need to sign some forms to authorize surgery. Here, here, and here.”
“Surgery?” I asked.
“Yes, we can’t get your fever under control. Our only choice is to go in and remove the cause of the infection. Otherwise your prognosis…we’ll it isn’t good,” he said in a quiet, somber tone. I understood what he was telling me and started signing the forms.
“I need to tell you of all the possibilities of having this surgery,” and he listed off the usual complications and issues and then added, “and you may end up with a stoma.” By this time another surgeon had joined the growing group at my bedside. She seemed to be in charge.
“May end up with a stoma?” I asked, “how likely is that?” The new surgeon answered, ” well, we never go in planning to create a stoma, but until we go in I can’t say for sure. They’s be coming to move you to surgery in a few minutes.”
The doctors disappeared and my nurse appeared to start prepping me for moving to pre-op. As she moved my IV bags the transport team came in. “We’re going to take you down to surgery now,” the nurse said. I grabbed my phone and sent a quick text to my brother. If something happened during surgery, I wanted someone in my family to know what happened while they slept.
In pre-op I was greeted by even more medical staff. One of the anesthesiologists started to ask me a slew of questions, a woman who identified herself as a nurse held my hand and spoke to me in a comforting manner, then I heard doors open, multiple footsteps and could feel the group around me stiffen a little.
“Mr. Wahr, I’m the faculty surgeon overseeing your operation. Here’s what’s happening. The fissure you have is worse than we thought. The contents of your bowels are emptying into your abdominal cavity, causing infection. If we don’t go in and stop this, we won’t be able to bring the infection under control. The outcome will not be positive. Do you understand?” I nodded that I did. “We’ll remove the damaged areas of your intestine and when you wake up you will have a stoma. Do you know what this is?”
“Yes,” I replied, “but it sounds better than the alternative.”
“It is,” the surgeon replied. “You’ll be going into surgery now.” And with that they began to wheel me to the operating room. I noticed the time on a clock. It was not even 5:00 A.M. They were not wasting any time which told me all I needed to know about the seriousness of my situation.
A quick trip down the hall, during which I mostly observed the ceiling, and we were in the operating room. A white, sterile looking space filled with equipment and a woman sitting in the corner covered with a blanket around her shoulders. Part of the anesthesiology team perhaps? I’ll never know. A quick transfer from my bed to the “table” and the voice of the anesthesiologists who spoke to me earlier. “Are we ready? Okay, here we go.” A mask was put on my face and just as I was wondering if this was it and would I ever wake up, everything went black.
Next thing I knew, I heard a disembodied voice asking me questions, “Mr. Wahr, can you tell me where you are?”
“U of M Hospital, I’m having surgery.”
“Very good, everything went well. You’re going to a room now.”
I continued to drift in and out of consciousness for an unknown amount of time. It was about 10:00 A.M. when I finally seemed to actually wake up. I said a silent prayer thanking God for letting me wake up and yet another doctor came into my room. This, I would later learn, was the “attending” doctor for the intensive care unit I was in.
“Mr. Wahr? How are you doing?” he asked.
“I guess fine. Considering.”
“Yes, I understand. The good news is that the surgery went well. You do have a stoma, but the infection and fever are gone and you should make a full recovery. You were lucky,” he paused to consider his words carefully, “this was the kind of thing that people die from.”
“So I hear.”
He went on to tell me a little more about the surgery and that the surgeon would be in later to check on me (as he did each day I was at the hospital). He then left me with the nurse so I could settle in.
Thus begins my newest adventure with Crohn’s. In a way I always suspected that this day was in my future – yet it was still a surprise when it happened. Many Crohn’s patients end up in surgery and with stomas. I’ve managed to avoid it for more than 30 years so in that sense I’ve been fortunate. And there is the possibility that in 6 months or so, presuming that the Crohn’s is under control, that I could be “hooked back up” so that my colon can be useful again. So, all in all, I’m handling the situation pretty well.
My current concerns while I recuperate and adjust to life with an appliance attached to my side (which does get changed every three to four days): 1) dehydration – most of the water for the body is absorbed by the colon. It will take time for my small intestine to realize it needs to pick up the slack; 2) weight loss – even though my appetite is good, food is still passing through my intestine too quickly. As a result, I’ve been slowly losing weight (almost a pound a day). Something a lot of folks dream of, but be careful what you wish for. When I was first diagnosed with Crohn’s I dropped down to about 140 pounds from my then previous weight of 180 pounds before being stabilized. I sure don’t want to be that thin again. Plus, all the weight seems to be disappearing from my chest and shoulders and thighs. Not my belly where I really don’t need it. Muscle loss is certain at this point. There goes the last 30 years of training down the drain; 3) infection, which I’ve avoided so far, always a risk after surgery but especially for someone with a weakened immune system; 4) controlling the Crohn’s. My past medical regimen didn’t prevent the fissure which is an indication that the treatments weren’t working. The interesting thing now is that my Crohn’s has historically been localized to the ileum. Now that my ileum, about a meter’s worth of small intestine, is gone the question is will my Crohn’s flare up somewhere else?
That’s it in a nutshell. I’m managing to deal with the appliance pretty well so far with only a couple mishaps (one in the doctor’s office) and I’m looking forward to returning to work soon.
Of course, I’ll keep blogging about my experience in the hopes of helping someone else with the same or similar situation. There’s always hope folks and we are all in this together.
On a side note, I had an interesting experience that was repeated with three nurses as they prepared to give me an injection in the back of my arm. It went something like this:
“Left or right arm?” the nurse asks.
“Doesn’t matter. Left.” I reply.
“Okay,” takes my arm to prepare the injection site. Stops and says, “oh, I’m not sure what this is. Is there a tumor in your arm? Or is that your tricep?”
“I hope it’s my tricep.”
“Yes, I guess it is. Not used to seeing a tricep like this. Very impressive.”
Now, I can’t be sure if the comment – from three different nurses – means I have an oddly shaped tricep or if they just don’t expect a relatively well developed tricep on a…ahem…mature man (though I think it’s looking pretty puny right now). I’ll go with the latter as it makes me feel better about myself. You have to look for the positive in every situation after all.